|
The Book Movement just came to life. Here's a recap: Gray Cook on Profiling Movement
"We have risk factors for every organ in the body...except the neuromusculoskeletal system" "Don't change your system, just throw a movement competency system in front of it" "Movement pattern atrophy...it's possible"
"Don't be tied to your methods...be tied to your systems and principles". Phil Plisky "It's not about the natural history of pain and injury, it's about the recurrence rate" Kyle Kiesel on the Functional Movement Screen
Greg Rose & Gray Cook on the Selective Functional Movement Assessment
"Our diagnostics (our thought process and clinical decision making) is just logic"
The Rules of Screening
"It's not magic, it was just a stability problem".
"Never bring a mobility problem to a stability correction...DON'T BE A ROOKIE!"
Kyle Kiesel on Pain and Motor Control
"We don't need more injury prevention programs, we need a better system" - Phil Plisky Mike Voight on Breaking Down Function “If you train the muscle you may not completely develop the movement, but if you train the movement the muscle will develop appropriately!”
SFMA Breakouts 101
Greg Rose on Functional Training
The Functional Continuum
The 4x4 Matrix for Reloading a Stability Problem 4 Functional Positions
4 Functional Exercise Resistances
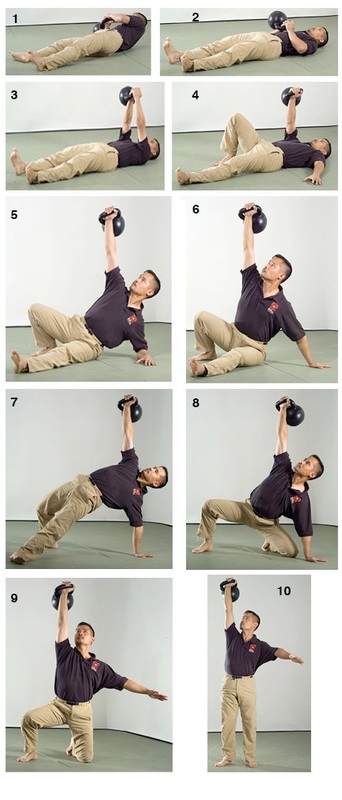 1-4 = 1/4 7,8 = 2/4 9 = 3/4 10 = 4/4 "Rookies only do 4x4's"
"Isn't it a better idea if I just gave you a philosophy and you make up the exercises?" Final Objectives
0 Comments
Leave a Reply. |