|
The following is a review of several of Craig Purdam’s presentations on tendinopathy at the recent 2011 Pan Pacific Conference for Medicine and Science in Sport, held in Honolulu. Craig is the head of physical therapies for the Australian Institute of Sport and had a wealth of information to share during the weekend. I was very grateful to be in attendance. Craig proposed that the pathology and the response to treatment are different in the various tendinopathy presentations and therefore interventions should be dictated by the specific pathology. More specifically, that there exists a continuum of tendon pathology. Namely:
Craig stressed that rather than looking at the above as three distinct phases, that a continuum should be kept in mind. 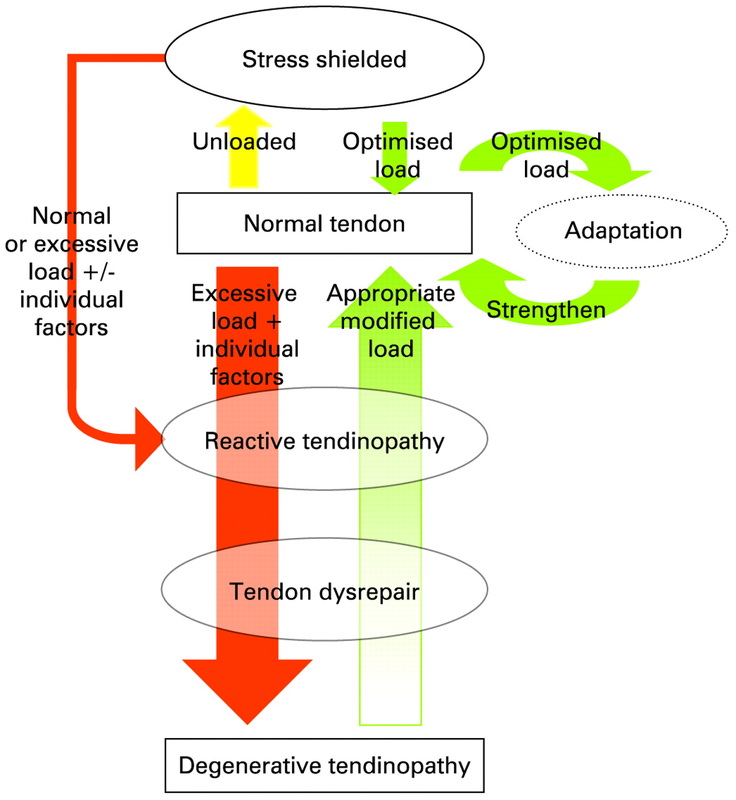 http://bjsm.bmj.com/content/43/6/409/F1.large.jpg. Classification of Stages must be identified via:
Stage characteristics: Reactive Tendinopathy
Tendon Dysrepair
Degenerative Tendinopathy
For ease of interpretation, the above continuum is divided into:
Cornerstones of Rehabilitation:
Considerations:
Rehabilitation Principles:
Treatment Strategy: Reactive Tendinopathy:
Tendon Dysrepair:
Degenerative Tendinopathy:
*Note modalities such as cross-friction, therapeutic ultrasound, and shockwave are only appropriate in the Late Tendon Dysrepair and Degenerative Tendinopathy Stages *For (hopefully) obvious reasons, I have intentionally omitted recommendations pertaining to pharmacological treatment.. Purdam has authored and co-authored numerous articles on tendinopathy but perhaps three of the most significant ones you may be interested in are:
0 Comments
Leave a Reply. |