|
As a medical practitioner trained in the Advanced Selective Functional Movement Assessment, I recently had the privilege of attending the Functional Movement Systems' internship program. Held in Evansville, Indiana, this 3 1/2 day workshop was a means to train specific practitioners in the overall integration of the Functional Movement System.  Having integrated their systems into both athletic and clinical practice over the past several years, I felt it was necessary for me to attend the internship to fully understand the goals of the "system", particularly since one of my objectives is to perform risk identification research here at the University of Alberta in the near future. While this was certainly a comprehensive internship, my goal here is to provide you with a brief review of my internship experience. To start off, I will first admit that while I have been using the SFMA for quite some time, there have been many instances where I have "broken the rules". So one of my objectives coming into the internship was to truly understand when breaking such rules is ok and when doing so may be a bad idea. Take for example the treatment-based classification for low back pain. Research has demonstrated that there may be instances where manipulation, stabilization exercises, and other treatment strategies are appropriate for patients presenting with low back pain. Now if you're familiar with the SFMA, you'll understand that often your assessment will lead you to areas away from the region of pain for the purposes of correction and treatment. So taking both of these into account, should we indeed be breaking the rules and adhering to the TBC or should we strictly follow the SFMA. Well based on our discussions during the internship, it basically comes down to this: "The rules are there to keep you safe when you don't know what you don't know...that ultimately, you just need to know why you got to where you got" Many of you who FMS trained will know that the FMS is a tool used to aid in predicting injury prior to participation in athletic activities. You will also know that the objective of the FMS is to identify movement pattern dysfunctions that may lead to injury through identifying an athlete's (in)ability to perform 7 specific movements. What you will also know however, is that the FMS has come under intense scrutiny in recent years not only due to a misunderstanding of its role in clinical scenarios, but also due to its use for anything other than its true objective. Specifically, it has been criticized to lack both a measure rotational competency as well as end-range, dynamic stability and as a result, many professionals simply aren't convinced. Ultimately, my goal here is not to change one's mind but simply to introduce the Y Balance Test. The Y Balance test was covered heavily in this internship and since I was relatively unaware of its role in the overall system, I can honestly say that learning this test has really opened my eyes and mind to the role it plays in the identification of injury risk. Incorporating both an upper and lower quarter component to end-range, dynamic stability testing, this test now occupies a large space in my shed. Through its combination with the original FMS, as well as the software by move2perform, I really and truly think that this system holds a lot of power in identifying an athlete's future risk of injury. To put it simply, the Y Balance Test seems to be an excellent predictor of risk (at least in the current literature) while the Functional Movement Screen tells us why and how. Now combine this with a previous history of injury, the athlete's sport and age and boom...you have an excellent algorithm for risk identification. Oh wait, this already exists with the move2perform software! One of the highlights of the internship was an evening kettlebell session with Paul Gorman, ATC, RKC, CSCS. As someone who uses kettlebells but has never been formally trained, this was an excellent learning opportunity for me to truly understand its role in the rehabilitation setting. Paul spent plenty of time teaching us methods for progressing the Deadlift, Swing, Turkish Get Up, and Goblet Squat. Specifically, he broke each of these movements down to their component parts and really elaborated on what we should be focusing on when working with our clients and athletes. I can provide you with all the specific details here but I truly believe that formal training is a more responsible form of learning that a simple blog post. What you should note however, is that adherence to proper progressions is the key to kettlebell training. That said, here are some images from this KB session.    Taking things back to the FMS, another highlight of this internship was a conference call / webinar with Rob Butler of Duke University. Rob has been heavily involved in FMS research as of late so this was an excellent way for each of us to truly understand the literature behind their system. Aside from providing us with a comprehensive review of the current literature as well as studies in progress, Rob also provided us with some notable quotes that really shed some light into what we are dealing with. "MDs want and MRI...I want an FMS, SFMA, and Y Balance" "Why is a dysfunctional deep squat a medical emergency at 2 years old but not at 14 years?" "Can we upload a better motor program?" "We need to clear fundamental movement...'but it hasn't been shown in research'...ya, but what else has?" "FMS & Y Balance, the portable gait lab" "When you screen someone, you're telling them something they already know...but now you're objectifying and quantifying it" "Y Balance - to test for if...FMS - to test for why" Another significant component to this internship was the application of the system into our everyday practices, be it the athletic or clinical setting. Each delegate was to present a case study where the group was to both critique and provide recommendations to enhance our learning. Interestingly, Kyle also provided us with a rounds type of case presentation that to our benefit, resulted in the incorporation of dry needling in treatment. One of the delegates was a therapist from kinetacore, so he was kind enough to demonstrate the use of needling in a live scenario. The video below is not of the actual case but of another delegate receiving treatment for a neck complaint. Overall, this internship was a success for me as a practitioner at this current stage in my career. Again, my objectives for this course was not only to truly understand the system in its entirety, but also to solidify my understanding of patient management based on my current knowledge of the existing research as relates specifically to the functional movement system as well as sport medicine in general. Most certainly, one can hold a successful practice without ever taking any of these courses, however, for me, any opportunity to further myself as a clinician is just icing on the cake. If you're interested in specific details of information that really resonated with me over the week or simply want more information of any component of the functional movement system, you're more than welcome to use the comments section below.  Apparently women don't like the SFMA?
0 Comments
Typically upon attending a course, workshop, seminar or conference, I write a recap not only to share information with all of you, but also to review what I have learned. This process generally facilitates a better understanding of the concepts covered and allows those reading to gain a better insight into specific courses that they may have yet to take. Here are several examples:
This past weekend, I had the opportunity to assist Dr. Liebenson with his Functional Capacity Evaluation & Performance Enhancement workshop hosted by MSK-Plus.  Assistant Instructors: Drs. Gabrielle Shaughness, Jason Brown, Rob Block. MSK + host: Dr. Glen Harris. Dr. Craig Liebenson. Assistant Instructors: Drs. Jeff Cubos, Scott Champan, Ryan Van Matre (missing) This review, however, will be different. Rather than writing a review of the workshop itself, I thought it would be important to provide you with a video of Dr. Liebenson eloquently describing the clinical approach to treatment and rehabilitation. I hope this provides you with a better understanding of the important role the Clinical Audit Process plays in effective patient-centered care.  Finally!
It took me a while to get through all of Charlie's educational dvds but I did. Will admit that I have to watch each disc several more times to soak up all the information but for those of you who have yet to check it out, I suggest you do so asap. As a strength coach, an athletic trainer and a physical therapist Charlie shares a wealth of information in his recently released dvd set, Training = Rehab Rehab = Training. On top of that, he's been a competitive powerlifter and an RKC in training so he definitely walks the walk. This is an important point to realize since while many clinicians often restrict clients and athletes from performing specific exercises for "safety" purposes, Charlie has both put himself under, as well as lifted, hundreds of pounds of load and truly understands the human body's true capacities. That is not to say that this dvd is meant for the hard gainers. It very well could be, but I'd say its for anyone involved in a training or rehabilitative capacity. It simply illustrates the fact that when he tells a trainer to "back off and refer out", he truly means it! Here's a little Q & A where I asked him to delve a little bit further on some of the principles he espoused. 1) Charlie, in the dvd set you quoted several times that "Stability is the ability of a joint system to control movement in the presence of potential change" The working continuum of spinal stability training from the Spine Control Symposium that I attended in Toronto stated that based on the load (high vs low) and speed (slow vs fast) of a given scenario, a certain amount of stiffness (high vs low) is required. For example, situations that are slow in duration and high in load require high stiffness - think squats and deadlifts. Would you consider this similar to your thought process of “stability” and if not, perhaps you may describe how your definition may differ? "Keep in mind, this definition of stability is more contextual to begin the understanding of human movement. It is important to understand that stability can come from many different components and strategies. Some are desirable and have tissue integrity, while others are degenerative. This can be the movement in general like repetitive touching your toes or relying more on bony approximation in a deadlift that meets a visual marker of integrity. Stiffness is definitely a friend to maintaining stability as one of the potential components adding to movement integrity. I would be cautious to rely overly on muscle tissue stiffness for spinal stability if it inhibits segmental stability. I believe we need both.". 2) You also mention that “the painful joint is usually doing something right” and that "the hip has more to do with ankle sprains than the ankle”. I think this really sums it up. Many of us have heard of Mike Boyle’s noose example, but ultimately it comes down to the statement you made above. You also mentioned that “the knee is stupid”. Many of us are aware of the influence the “core”, hip, and ankle have on patellofemoral stability and while minibands and Cook bands are quite widespread in the rehab industry, my guess is that you utilize a strict, no nonsense approach to patellofemoral rehabilitation. I’m sure you do use the above equipment but are there others in your toolbox or are you simply strict on form and focus on progressions? "I definitely use the bands, and I definitely devalue the knee proper in terms of rehabilitation. That being said, it is critical to restore patellar mobility when it's deficient, and there are some rotational mobilizations that can restore centration to the knee. Also far too often, knee pain that lingers or tough to crack is a function of compression of the patella as a result of rectus femoris tone that is quickly treated with IASTM. This approach though is more treating the hip musculature than the knee.". 3) On the “Core Pendulum Theory”: When discussing this theory, do you simply mean the proprioceptive input involved at (normal or pathological) end range via the joint capsules and ligaments? Or are you implying mid-range input from the muscules and musculotendinous junction as well? This is may be a rhetorical question, but an important one nonetheless. "I am implying both. I believe the receptors through joints, capsules, muscles, tendons, etc. yield information to the brain that shifts neural flow away from tonic muscles and towards phasic muscles. My theory is that regardless of the individual joint position at a given time, the mechanoreceptors "know" the mid- and end-range capabilities of the joint. Those "conversations" govern the local stability of the joint based on a "need" basis. If the joint can stabilize off tone and neurally driven stiffness, local stabilizers are inhibited." 4) Being trained in Ontario, many of my colleagues are well versed in the concept of “bracing” the core in order to achieve spinal stability. However, being familiar with the work of those in both Australia and Prague it seems as though there may be a requisite precursor to this approach. Would you mind briefly discussing the “High Threshold Strategy” and the neurological and physiological rationale to targeting the inner and outer core in rehabilitative and corrective exercise? "A High Threshold Strategy is based off Hodges nomenclature that buckets 4 levels of stability patterning. I forget the name of the first local pattern, but it is just a visualization of muscles activating. Local stabilization is the rank and file low load training that they believe in like draw-ins and multifidus training. This is the inner core cylinder where I believe is managed by the diaphragm feeding forward to the TA, multifidus, and pelvic floor. Obviously others are comfortable with the TA or other pieces driving the pattern. Global Stabilzation is the plank series, push-up, heavier diagonal patterns, the tried and true McGill-like training. Global Mobilization is the foolishness such as crunches, supermans, movements that involved repetitve and loaded movement of the lumbar spine. Champions of the Queensland methods I believe espouse this type of training which varies in my mind from unfortunate to nauseating. Based off the solid research of delayed onset of the inner core (local stabilzers) in the presence of pain, there is a parlay of overactivity of the outer core (global stabilzers). This is a high threshold strategy, when the globals and not "balanced" with the activation of the locals. This is actually very consistent with Janda's message in as much as the globals such as RA, obliques, QL phylogenetically are phasic muscles, and the locals are tonic. The High Threshold is when the tonics are inhibited, and phasics are facilitated. The key to appreciate is that after the pain is remediated, the high threshold strategy often remains and fouls ideal movement. I do not believe that harnessing the body's full "juice" for loaded and powerful patterns is possible without the inner core stabilizing in sequence and allowing for the phasic muscles to deliver. These patterns can be retrained, sometimes quite rapidly." 5) You introduce the Selective Functional Movement Assessment with restrictor plates. Basically this is the top tier, 7 tests in the assessment technique used to guide manual therapy and rehabilitation. My question is this. If you are suggesting that performing the breakouts should only be performed by clinicians, why not simply utilize the original FMS?” "I believe Gray wrote in Movement that you actually can use the FMS to treat pain. I would suggest you must be on your game and quite skilled to be able to cull out if it is pain causing bad movement or bad movement causing pain. Also consider that the deeper screens to the FMS are designed to bucket mobility vs. stability fixes. When there is pain, it is still challenging to always discern if you are seeing a limitation of some level, or if it's pain creating the situation. You may be able to diffuse the pain, and the limitations fixes. Or it may not fix. My goal was to establish a common language in terms of non-medical clinicians and medical clinicians working off of the same template without dishonoring the natural and logical boundaries between the 2 skill sets. Many trainers don't or won't refer out for somewhat fair reasons. I believe what I presented was a fair and honest way to provide those individuals, along with a whole host of other valuable information, a way to not screw up the situation if they choose to work with someone in pain. Referring out is the best approach, which I believe is something I might have mentioned more than 6 times on the DVD. That is the bigger take-home rather than this SFMA with Restrictor Plates." Many thanks to Dr. Weingroff for taking the time to answer these questions. If you yourself have any questions for Charlie, feel free to let me know or contact him directly through www.charlieweingroff.com. The following is a review of several of Craig Purdam’s presentations on tendinopathy at the recent 2011 Pan Pacific Conference for Medicine and Science in Sport, held in Honolulu. Craig is the head of physical therapies for the Australian Institute of Sport and had a wealth of information to share during the weekend. I was very grateful to be in attendance. Craig proposed that the pathology and the response to treatment are different in the various tendinopathy presentations and therefore interventions should be dictated by the specific pathology. More specifically, that there exists a continuum of tendon pathology. Namely:
Craig stressed that rather than looking at the above as three distinct phases, that a continuum should be kept in mind. 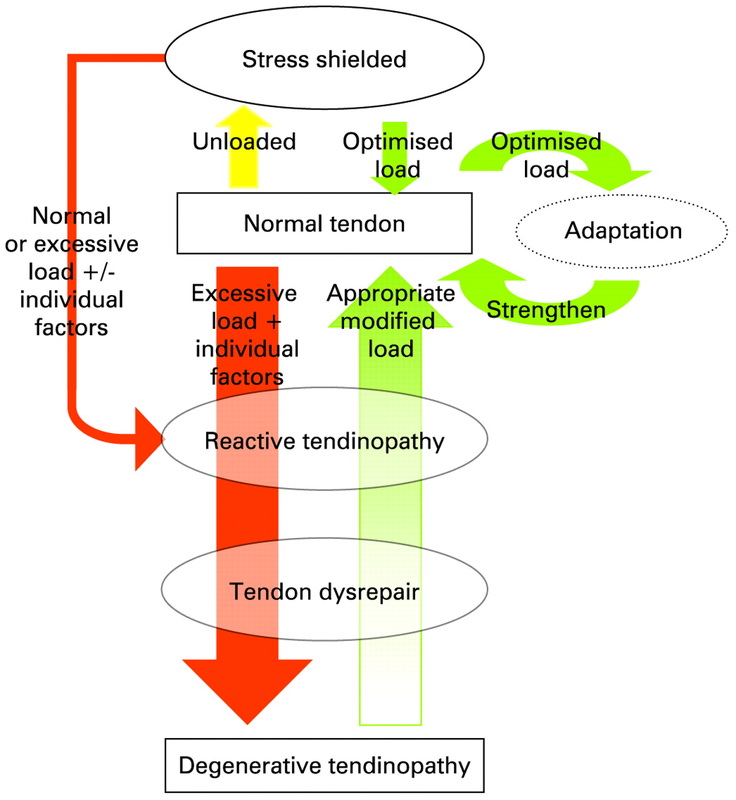 http://bjsm.bmj.com/content/43/6/409/F1.large.jpg. Classification of Stages must be identified via:
Stage characteristics: Reactive Tendinopathy
Tendon Dysrepair
Degenerative Tendinopathy
For ease of interpretation, the above continuum is divided into:
Cornerstones of Rehabilitation:
Considerations:
Rehabilitation Principles:
Treatment Strategy: Reactive Tendinopathy:
Tendon Dysrepair:
Degenerative Tendinopathy:
*Note modalities such as cross-friction, therapeutic ultrasound, and shockwave are only appropriate in the Late Tendon Dysrepair and Degenerative Tendinopathy Stages *For (hopefully) obvious reasons, I have intentionally omitted recommendations pertaining to pharmacological treatment.. Purdam has authored and co-authored numerous articles on tendinopathy but perhaps three of the most significant ones you may be interested in are:
A guest post from my good friend and colleague, Dr. Thomas Lam of Fits Toronto
After the first talk by Robert Schleip I could have left and felt very satisfied with attending the conference. WOW. But I’m so glad I didn’t! This conference helped solidify some thoughts and completely open my eyes for a new ways of thinking. Without question there are way too many highlights to write about in a single blog post. So I’ll write about my TOP 8 Highlights. Originally I was going to post highlights of each speaker, but because there were many commonalties between the talks I’ll instead write about the major highlights echoed throughout the conference. A special "thank you" needs to be delivered to Dr. Glen Harris (MSK Plus) and Dr. Wilbur Kelsick (Maxfit Movement Institute) for making this conference happen! I’m so happy that I attended that I’ve already sent my RSVP for the 3rd International Fascia Research Congress. TOP 8 highlights: 1) Our Anatomy is WRONG! Open any text book and you’ll see clearly defined muscles, tendons, nerves and blood vessels. Each tissue can be clearly seen. But where’s the fascia? Fascia is our tendons, ligaments, and all of our collagenous connective tissue that connect all our structures in our body into a single body. Forget about your knee bone is connected shin bone. The reality is more like your knee bone is connected to your ear! 2) You might not be stretching what you’re stretching? Based on the organization of fascia, Vleeming researched the strain transmission that occurs with a straight leg raise. Incredibly the iliotibial band and the lumbar fascia compared with strain to the hamstrings is 240% and 145% respectively. This occurs because fascia is multi-directional and a large portion of the strain that occurs during a straight leg raise is transmitted laterally. To further illustrate this check out Plantar Fascia Magic. 3) BRAIN POWER – Separate the forest from the trees. Our brain is the central processing center of our body. There are over 80,000 sensory inputs per second that enter our brain that must be processed to formulate and make fine adjustments to our movements. Note I didn’t say proper movement. Developing sound movement patterns takes time, based on deliberate training principles that address key movement qualities. This is without question the Forest. It’s the big picture that we must always address. It’s the key factor that determines injury rates and sport performance. The forest is made up of many components, but they are the details. Some details are more important than others. In this analogy fascial issues range in how they impact our ability to perform movement. Some fascial problems would be large trees, but some would be like a shrub, others could be like a blade of grass. But never mistake that it’s how we process and develop our movements that determines injuries and performance. This concept is surprising lost. Many health care professionals focus on the details beautifully but miss the big picture – THE FOREST. We must always aim to improve our movement qualities by address the most effective and efficient detail. 4) Running Shoes and Orthotics – WOW! I really have to think about the implication shoes and orthotics have on injuries and athletic performance. Currently many people are subscribing to the concepts of Bare Foot Running, popularized by Born to Run (you gotta get this book – it’s amazing), Chi of Running, Pose Running, Vibrams and Barefoot Ted – just to name a few. I’ve known about this concept for a couple of years, but after reading Born to Run, attending this conference, and recently speaking with Dr. Larry Bell the merits of bare foot training are more salient than ever. 5) Stretching and Conditioning Fascia – Let’s get Crimped. There are many methods that need to be integrated to effectively condition our fascial system. Yoga by itself is not enough, nor is strength training. Yes strength training is important to condition your tendons and ligaments. In fact, the tendons of those that don’t strength train lose their elasticity and tensile strength properties. If you examined their tendons compared with a well trained athlete you’ll see that their tendons are straight compared to crimped. You really want crimped tendons because those have enhanced elastic properties. These properties aid in elastic recoil and you become faster and more explosive. Stretching and flexibility have long been known to help with fascia pliability, but they are not enough. Based on the multi-directional layout of fascia (see point 2) we need not only spiral patterns to address the multi-directional layout of fascia but we need active muscular contraction combined with spiral patterns to address all fascia bands. I’ve been playing with this concept for some time with end-range oscillation techniques. 6) STRETCH ONE HOUR BEFORE COMPETITION. Research on stretching and power has made many afraid of stretching. But there may be more to add to this picture and it might change the minds of many strength and conditioning professionals about stretching. While stretching squeezes out matrix hydration, which contributes to the decrease in subsequent force production, after 1 hour we see a supercompensation of matrix hydration which enhances force and power production. This means if we stretch one hour prior to competition we’ll be in a heighted state of elasticity! Gymnasts have been utilizing this approach for years and the common ancient practice of wetting a rope repeatedly to raise an Obelisk further illustrates this power property of water and mechanical properties. For those of you as curious as myself as to what an obelisk was 7) We’re ANTELOPES! We have the same elastic properties as an Antelope! Elasticity is the ability to use energy. We’ve talked about this process at length in our four part series about Reactiveness and Stiffness. This ability is a huge quality we develop at FITS and its mind blowing to learn that we have the same elastic properties as an Antelope bounding in the African Saffana. 8) THE SAIL AND MAST – Mechanoreceptors in our superficial layer of fascia are our most abundant and perhaps our most sensitive prioprioceptors. I’ve been taught that our self-awareness of our bodies in space (prioprioception) is based on the integration of information from our eyes, vestibular apparatus (housed in our ears), and joint mechano-receptors. Interestingly, research has shown that joint mechano-receptors are active near to end range. But what happens in between???? It appears that mechanoreceptors in our skin are in the perfect position to serve this function. The analogy that Dr. Schleip used was a sail and mast. While the mast only moves slightly the sail is incredible sensitive to changes in the wind. BONUS!! “Any hockey player that becomes concussed will have a hip or hernia problem” – Mark Lindsay Thanks for reading… I look forward to exploring these concepts in more depth in the near future stay tuned. In the meantime here are some great resources regarding fascia. This list is by no means complete. RESOURCES: Robert Schleip. This website is easily the most well linked site on fascia. The amount of great content about fascia is staggering. If you’re interested in learning about fascia you MUST CHECK THIS SITE OUT: http://www.somatics.de/somatics.html Journal of Bodywork and Movement Therapies. The journal is a great resource for healthcare practitioners. http://www.sciencedirect.com/science/journal/13608592 Fascia Research Project. This site highlights the amazing research being conducted out of Ulm University. http://www.fasciaresearch.com/ 3rd International Fascia Research Congress. http://www.fasciacongress.org/2012/ Stretch to win. I really like this technique. I’ve had the pleasure of meeting Ann and Chris Frederick and they’re amazing. This is a great approach that integrates many proprioceptive neuromuscular techniques from all around the world. http://www.stretchtowin.com/ Rolfing. While I don’t understand too much about Rolfing I’ve met some great Rolfers who have really changed my thinking so I believe there is a lot to learn from them and their techniques. http://www.rolfing.org/ Carrick Institute for Clinical Neurology. I know of three great health care practitioners (Dr. Mark Linsay and Sam Gibbs) that are enrolled in this program and I’m most likely going to enrol shortly. http://www.carrickinstitute.org/ Thanks, Dr. Lam! Highly encouraged by Drs. Liebenson and Weingroff, two well regarded rehabilitation professionals, I had the opportunity to attend the Prague School's Dynamic Neuromuscular Stabilization "A" course this past weekend in Azusa, California. Dynamic Neuromuscular Stabilization, or "DNS" as it is commonly referred to, is a manual and rehabilitative approach to healthcare grounded in the scientific principles of developmental kinesiology. One of the key tenets of this approach is the activation of the "integrated stabilizing system" in order to facilitate optimal functioning of the locomotor system. This particular course was primarily instructed by Clare Frank, co author of "Assessment and Treatment of Muscle Imbalance" and Prague-based physiotherapist, Lucie Oplova. As I mentioned above, this approach to rehabilitation focuses primarily on the activation of the integrated stabilizing system of the spine. That is, the short intersegmental spinal muscles, the deep neck flexors, the diaphragm, the abdominal wall, and the pelvic floor. Many of you may be familiar with the research from Australia indicating the importance of a "feedforward mechanism" for spinal stabilization, and while we may not be convinced of the Transversus Abdominis in being the only important muscle for such mechanism, this approach views the relative interplay of the above musculature as being integral in the stabilization of the spine. In fact, even more important may be the control via the central nervous system (CNS). Postural ontogenesis and developmental kinesiology, or the development of muscle function for short, is directly related to CNS maturation. The absence of such maturation or the presence of its disturbance, forms the basis for such neurological pathologies as cerebral palsy. Such conditions typically manifest itself in predictive (aka not random) presentations, resembling functional musculoskeletal pathology we are so commonly familiar with in the modern day lifestyle.  As a result, it seems evident that the majority of the dysfunctions we so commonly see may be more related to higher level central nervous system functioning than we give credit to. Therefore it is important that rather than taking a local approach to "muscle activation", we must take a higher approach of CNS engagement. In doing so, we must also pay attention to muscle coactivation patterns such that the optimal balance of said patterns results in functional joint centration. Joint surfaces that are well balanced ensure maximum load bearing is possible. Note: This likely goes hand in hand with individuals who have difficulties performing the squat maneuver. Commonly we think of a "tight this" and a "weak that" but far too often we fail to realize that this dysfunction may simply be a de-centration of joint surfaces and subsequently, the brain telling that individual that perhaps he or she should not be performing a squat until such joints improve their dynamic positioning. Absolutely muscles are under complete control by the brain but how often is the central nervous system our area of corrective focus? Therefore, optimal muscle functioning will shape structural maturation (think denerative joint disease) and optimal muscle functioning is based on central nervous system maturation. Remember that the CNS is plastic (or elastic for those of you familiar with Lorimer Moseley) so while someone may have experienced (perceived) optimal development it certainly does not immunize them from dysfunction later in life. Program (CNS) - Function (muscle) - Structure (bones, joints, etc) For those of you familiar with movement patterns, according to the DNS approach they are simply a window to examining what occurs at the CNS level. Think about it, problems that we commonly see generally resemble primitive patterns. (Think protective guarding after a shoulder injury). Since such postural and functional pathologies mimic developmental maturation and insufficiency and since developmental kinesiology follows a system of sagittal stabilization prior to frontal and transverse stabilization, then it seems reasonable to follow this approach from a rehabilitation and training perspective. And so while the DNS approach attacks active exercise in three critical positions...
...it is prudent that we take the same approach in the methods we employ. This in fact is one reason why I have incorporated the SFMA approach in practice. But for those of you familiar with the SFMA, the DNS system fits in quite well, especially in those cases where your patients suffer primarily from a fundamental stability deficit. Heck, I’d even be so bold to suggest that the DNS system would fit quite well in the corrective strategies of the FMS. Say it with me; “Proximal stability for distal mobility”
This does not mean that we must take a mobility problem to a stability fix. Dr. Weingroff states this clearly in his DVD. But optimal (local) mobility will precede optimal (local) stability. And optimal (proximal) stability will facilitate optimal (distal) mobility. But we do have choices. If integrated spinal stability is warranted, we can train it with any means we choose. We can train the ISS in any of the three suggested DNS approaches. We can train the ISS in the most dysfunctional, non-painful movement pattern. We can train the ISS in 1’s and the asymmetries. We can train the ISS in the McGill Big 3. And the list goes on and on. Just remember, as soon as you have it, you must move on to the next pattern. Go after it. Get it. Move on. In hearing about the DNS approach, you may have come across discussions pertaining to reflex stimulation. It should be stressed that reflex stimulation is only a part of DNS. Reflex stimulation (aka the voodoo) is simply a technique utilized to elicit pre-programmed movement patterns and achieve joint centration. As with other manual therapies, reflex stimulation can be thought of as rebooting the system. CTRL - ALT - DEL. But what about training the brain? I have mentioned this before and I’ll mention it again. In order to access cortical plasticity, the individual must perform the most appropriate exercise along the specific corrective continuum that is most challenging but also one that they can still perform quite well. This is training the brain. So reflex stimulation can be thought of as the jumper cables and active training of the most difficult yet appropriate exercise that they can perform well is letting the car run after the jumpstart. Click here to watch an introductory video on DNS "Zones of Support" and the "Punctum Fixum" as taught by the DNS are the specific areas where movement begins. The direction of muscle pull, in general, project toward these regions and the choices of support zones that our body makes depend on the initial position of that body. Thus, such "fixed point" will be dictated by whether a specific movement pattern is of the open chain or closed chain varieties. Additionally, as Dr. Kolar states in Dr. Liebenson's text, "Rehabilitation of the Spine", “The muscle may not be weak in itself, but it may not function well because its attachment point is insufficiently fixed. A muscle must have a punctum fixum.” Finally, one of the concepts of this approach that I felt was of great importance was the test and re-test. The identification of the faulty movement pattern, the correction, and the subsequent reassessment. This is the clinic audit process. Because as Karel Lewit states in his text, "There is no clinical field in the whole of our experience in which the purely clinical examination plays such a decisive role..." I cannot thank Drs. Liebenson and Weingroff enough for recommending this course, especially under the tutelage of Dr. Clare Frank. I have read Dr. Kolar's chapter in Dr. Liebenson's text, have looked at the literature on the Prague School website, and was introduced to some of their testing methods at Dr. Liebenson’s course. Yet while the information learned over the weekend was still relatively novel, at no point did I feel lost. The information was well presented and I cannot wait to integrate this approach into my current regime of care.  Instructors: Clare Frank, Lucie Oplova, and Kathy Kumagai
Below are my notes from Dr. McGill's "Building the Ultimate Back" workshop hosted by MSK+ on November 20-21, 2010. A total of 32 pages of notes were taken throughout the weekend. Prior to reading the following, I kindly ask that you take two things into consideration:
Enjoy!  Page 1 Range of motion and strength do not necessarily correlate with recovery
"Build capacity within tolerance within an injury mechanism that is part of their sport"
"The Lats activate natures 'back belt'"
"Scientists set up experiments in order to find what they're looking for"
"The squat is a hamstring exercise until you get halfway down. Then it hits the glutes"
"What a stupid exercise!"
"The orientation of interspinous ligaments are backwards in English anatomy texts"
"Building strength too soon may keep people chronic"
"Abdominal hollowing is pathological"
"The spine will break at 18% less load in the morning"
"Stop treating your spine like a ball and socket joint"
 Pages 16-17 "Nuclear worms" respond well to McKenzie techniques...if there is adequate disc height left
"Patterns of herniation are patterns of repeated stresses which are patterns of movement patterns"
"There is no bad exercise...just bad form and inappropriate loading parameters" "Do you know one world class athlete who does crossfit? I don't, because training to failure repeatedly outpaces the opportunity for repair"
"The best QL training is to go for a walk"
"Follow the endurance pathway"
"The curl-up really isn't a curl-up"
"Don't train the failed tests, train the reason why they're failing"
"Core strength makes the impossible, possible"
 Page 32 What a powerful statement in the context of patient management. With the vast array of treatment techniques and tools flooding the market these days, it is quite easy to get caught up in feeling the need to get certified in this and credentialed in that. Here are a few to illustrate my point. Tools:
Several years ago, I had the privilege of attending my first Modern Spine Care workshop by Dr. Craig Liebenson in Seattle, WA. The workshop was hosted by Drs. Jim Kurtz (Seattle Seahawks and Sounders) and Ming Ming Su-Brown of NW Sports Rehab. What an awesome facility! "Modern Spine Care" however, was not about the tools...it was about the process. Integrating theoretical principles and practical applications from such pioneers as McGill, Janda, Lewitt, McKenzie, Kolar, Butler, Brugger, Cook, Gary Gray, Travell, Moseley, etc.. (seriously, he had them all), Dr. Liebenson provided us with a comprehensive, clinical reasoning framework upon which we should be managing our patients. Here are some of the principles that flipped my switch this weekend. The Clinical Audit Process:   This was the meat and potatoes of the weekend. So rather than providing you with my interpretation of such a valuable clinical reasoning and management process, I simply ask you to read the original document from DC Online. Just click here. Microbreaks The importance of microbreaks during rehabilitation and normal activities of daily living was strongly emphasized. Stuart McGill explains the importance of microbreaks in maximizing the margin of safety of our tissues in both of his texts (Low Back Disorders and Ultimate Back Fitness and Performance - both of which can be obtained from my Educational Resources page above) and Dr. Liebenson was very diligent in not only stressing the importance of such breaks but also implementing them within his workshop (we had to perform a toe touch and squat every 20 minutes). Two simple exercises to perform during these microbreaks to combat a sitting posture, for example, are reaching up to the air and the Brugger relief position (click here for a simple handout to provide your patients). The Importance of Self Care Since one of the most vital concepts in effective pain management is the utilization of graded-exposure to feared stimuli, the importance of implementing and facilitating self-care exercises cannot be understated. This may not seem new to most of you but here are some ways one can maximize its effectiveness:
 Functional Capacity Testing Since the goal of patient care is to close the gap between one's functional capacity deficits and their activity goals, Dr. Liebenson workshopped us through an excellent model for quantitative functional capacity evaluation. What was most interesting was that rather than reinventing the wheel, Dr. Liebenson simply combines those tests that already have normative data to compare to:
Random Thoughts from the Weekend
 On Saturday, August 28, 2010, I had the privilege of attending the spine control symposium put forth by the University of Queensland's Centre of Clinical Research Excellence in Spinal Pain, Injury & Health. This was a must symposium for all professionals in the rehabilitation injury who manage low back pain and with the constant growth and debate pertaining to the research in this field, I am truly thankful for such an opportunity to expand my knowledge. As such, I also believe that it is my responsibility to relay that information onto my colleagues and will make an attempt to do so below. Note: Please click here for Part 2 Please be aware that the following information is based on my interpretation of each lecture and therefore, may be subject to "lost in translation". 'Clinical Update: Emerging trends in exercise management of spinal pain' ~ Paul Hodges & Stuart McGill This lecture was the meat and potatoes of the symposium. Dr. Hodges was the main presenter and often asked Dr. McGill to provide some practical insight into some of his interventions for low back pain. While they both stressed that they were likely very similar in their approach to spinal care, it was evident from this talk that the divergence is still glaring. In fact, even the miracle blade could not cut the tension in the air although both were very professional in their "debate". Here are my notes: Basic principles:
5 basic but key components to DYNAMIC CONTROL:
Treatment Goals:
Posture: Dr. McGill gave an example of the importance of posture and its relationship with our breathing. Feel free to perform a self-assessment in the various positions
Movement: Dr. McGill also provided us with a movement correction example
*All three (posture, movement, muscle activation optimization) are important but we as clinicians have to figure out which of these is our priority in treatment." "STATIC STABILITY DOES NOT EQUAL FUNCTION" Interplay between dynamic and stiffness:
"Change in motor control is about looking at the whole system not the parts." Common features of motor control strategies: 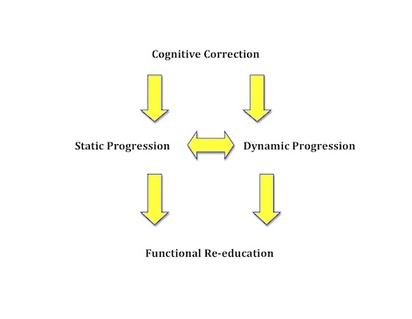 Dr. McGill on posture correction:
Preservation of feedback control may be via taping:
"NEUTRAL SPINE IS NOT STATIC!"
"The gluteus maximus is a (free) knee extensor!"
Activating the HIGH glutes & glute med:
Activating LOW glutes:
Posture and Movement is about load:
McGill on Bracing:
Hodges: There’s a difference between just making a muscle active (Transversus Abdominis) vs an optimal way of using the muscle:
Hodges: “There is no doubt that Stu and I have differing positions on the role of the deep muscles in the clinical approach but I think it is good that we have different ideas because all individuals patients are different.” "The Transversus Abdominis is not the most important thing in low back pain but our data show that it is the most consistent deficit in low back pain presentation. Therefore it is important to address this muscle as part of the comprehensive package of treating low back pain." "Improving the activation of the deep muscles may decrease the over activity of the global/superficial muscles." Dr. McGill on the Transversus Abdominis:
Dr. Hodges:
*In my opinion, It’s an apples vs oranges debate!" "Train movement control, posture and muscle activity during rehabilitation"
Dr. McGill: “Fix the biggest things first to get them out of pain...THEN fine tune!"
Dr. Hodges’ strategy of multifidus activation:
"There’s something about attention to detail that’s driving changes in neuroplasticity" Dr. McGill:
Dr. Hodges: "Delays are significant in a motor system."
As mentioned earlier, this turned out to be an interesting and enlightening high tension academic debate but both experts argue that it would be most valuable to have a patient on hand to both assess to really truly get an idea of how each think. They agreed that this would truly provide valuable insight into the magnitude of their agreement/disagreement. Out of all of this, they state that there is mostly convergence between the two and that it may be the last (5%)...i.e. their specific methods...that may be different. "Divergence is healthy. Because if not, what would drive research?" *The purpose of everything is the individualized goals of each patient. That’s it! On Saturday, August 28, 2010, I had the privilege of attending the spine control symposium put forth by the University of Queensland's Centre of Clinical Research Excellence in Spinal Pain, Injury & Health. This was a must symposium for all professionals in the rehabilitation injury who manage low back pain and with the constant growth and debate pertaining to the research in this field, I am truly thankful for such an opportunity to expand my knowledge. As such, I also believe that it is my responsibility to relay that information onto my colleagues and will make an attempt to do so below.
Please be aware that the following information is based on my interpretation of each lecture and therefore, may be subject to "lost in translation". Note: Please click here for Part 1 It must be stated that each of the two esteemed researchers prefaced their talks with addressing the fact that misconceptions often occur when one is asked to speak about a specific facet of their research. Both of them stated that the oft-requested material is simply a part of the big picture and as a result, labeling and misinterpretation typically occurs. 'Motor control changes in spinal pain: effects, mechanisms and efficacy of interventions' ~ Paul Hodges Adaptation & Rehabilitation: How does motor control change in the presence of pain? Some common myths explained (in red): The Transversus Abdominis and Multifidus are NOT the most important muscles for spine control
With respect to the debate surrounding the delay of motor activity with arm movement:
Motor control training is NOT just about training the Transversus Abdominis
People should NOT be encouraged to isolate the Transversus Abdominis and Multifidus in function
The need to isolate deep muscle activity in rehabilitation
Some explanations as to why motor activity decreases during pain:
Motor control isn’t always about giving people more…it may also be about taking things away
So does an increase in muscle activity during pain allow us to adapt? Yes! Is this adaptation about protection of the injured part? Yes – the high threshold strategy
Hmm... Adaptation ALSO occurs in the presence of a “threat” of pain
Adaptation may be good in the short term…but it may be detrimental in the long term
We have to match the system to the demands of the task! "Opinions on the links between back pain and motor control: The disconnect between clinical practice and research" ~ Stuart McGill A WHOLE BUNCH OF OPINIONS (in red) As mentioned earlier, Stu prefaced his lecture by stating that clinical groups develop preconceived notions of different researchers due to the requests they receive to speak about a specific component about their research.
"Its at the concentrations of stress where the tissues break down." "It is extremely important to ask if your patients have good days and bad days."
“People get painful backs because of the way they move”
Postural dominance:
Movement screening: "Just because they can (perform an ideal movement upon screening), it doesn’t mean they will!"
On using the term chronic non-specific low back pain: "Wouldn’t it be funny if we lumped all leg pain into “leg pain” and did a research study to determine the efficacy of various treatment approaches for “leg pain” (chiropractic care vs physical therapy vs massage therapy)"
“Muscles of the torso are fundamentally different than those of the limbs”
"The rectus abdominis, with its transverse tendons, is designed to create short range stiffness – otherwise God would have given us a hamstring!" Quadratus Lumborum vs Gluteus Medius for lumbopelvic stability in the frontal plane:
On the problem with performing a physical exam/assessment on a patient in jeans:
Internal vs External Focus for Skill Transfer:
Insert random quote here: “Pavel will kick you in the feet randomly and put you on your back before you even know it.” On the Transversus Abdominis: “Most clinicians would be more successful ignoring this muscle”
“I would be so bold to argue that Gluteal problems are much more dominant as a whole than the TVA”
On creating deep oblique training:
There you have it. A recap of the lectures presented by arguably the two most prominent leading researchers in the field of spine control. I apologize for withholding personal opinion from this summary, but I felt that doing so would provide everyone with an unbiased narrative of their lectures. |