|
0 Comments
One thing I'm trying to do more of is to say the word "don't" a lot less.
I've learned along the way that instead of saying "don't do this" or "don't do that", it's more effective to give the person in front of you an alternative action. For example, how often do the following work:
We are creatures of habits. And the research will tell you that in order to stop a habit you have to create a new one. Just think of when a toddler is crying. Children usually "move on" when you give them a candy, tell them a joke, etc rather than tell them "don't cry". The same with someone you know being stressed. Have you ever successfully told someone who's stressed not to be stressed? I haven't. And I find that patient under stress respond better when I explain that to them. They get the point and look for alternatives. And in coaching, if you're trying to get an athlete to perform a skill in a different manner, rather than saying "don't do ____", it's a much better (motor learning) approach to directly give them the alternative instead. Otherwise they'll continually cognitively focus on what not to do. Fighting fire with fire. It just doesn't work out well. So in essence, I'm not necessarily saying don't say don't. Instead what I'm suggesting is to do this instead. And "doing this" meaning find the alternative. This one will be short but I wonder if Manual Muscle Testing should really be renamed Postural Stability Testing?
During manual muscle testing, which is often if not always performed in an open kinetic chain manner, a "muscle" may demonstrate high strength or activation levels...and it may not. The local region tested may demonstrate a faulty pattern but so can the global / whole body pattern as well. We know (perhaps assume with high confidence?) that muscles need a fixed point in order to pull toward. If that fixed point is relatively "stable", then I would think that the potential for ideal neuromuscular output would be greater. But what if that fixed point is not actually "fixed"? That is, what if postural stability proximal to the region being tested isn't actually "stable". Would you get a reliable (let alone valid) reading? Also, what about the true function of the muscle for that given position in which it is being test? Tonic? Phasic? Reflexive? Support function? Stepping/Grapsing function? Do we even want full neuromuscular activity (hypothetical example: 100% MVC) in the first place? There goes the can of worms... I know many have already thought about this before and perhaps this was one of the things Janda was thinking about when he came up with his testing arsenal. But since it was currently at the top of my head, I thought I'd just blog about it. I was recently asked by a colleague what my opinion was on the most important tool (as a student) that she should put in her toolbox. To first give you some context, Katherine is a coach, trainer and strength & conditioning specialist who recently started chiropractic college. Fully knowing her professional background, I still intentionally gave her a bit of a difficult answer. I told her that experience, was single handedly the most important tool that she should put in her toolbox as a student. Let me clarify. In my opinion, whether you are studying to become a coach, trainer or clinician, you absolutely need to accumulate hours upon hours of working with people. It has everything to do with hard work. From figuring out what works and what doesn't and learning how to interact with people, to growing one's network and truly understanding what sacrifice and sweat mean in the real world, every student should start accumulating experience from day one. Be it volunteering, shadowing, or interning, experience is the fast track to separating oneself from simply being book smart. Because your clients, athletes, and patients will not only ask you how long you've been working but they'll also use the sniff test on you. And believe me, credibility matters. In an age where talking the talk is commonplace, the number of individuals who have walked the walk are relatively decreasing. Today, (face)book smart is reigning supreme. But unfortunately, those who are (face)book smart are also easy to pick out. Is it easy? No. But it's doable. Aspiring coaches, find a rake and rake the sandpit. Student trainers, turn on the faucet and fill water bottles. Students therapists, roll up your sleeves and get your hands on people. And young strength coaches, mop some floors. Go to bed hungry (literally and figuratively) and wake up tired. Trust me, having a diploma does not an expert make! "When you're earlier in your career, I think the best strategy is to just say 'yes' to everything. Every little gig. You just never know what are the lottery tickets." - Derek Sivers Remember:
 On November 16th I gave a lecture at the RCCSS(C)'s Run Faster Conference in Whitby, Ontario. The objective for my lecture was to put forth a therapists viewpoint of treatment integration into a performance enhancement environment whereby my goal was to suggest ways we can make 1% of our interventions 100% better. I started off by suggesting that every interaction between athlete and therapist is to be considered a “treatment” or more accurately, an intervention. That is, there is always an input - physical or not-physical, conscious or subconscious - with a subsequent output or adaptation by the athlete. Be it passive therapy, exercise intervention or communication, there will always be an after effect of each encounter. It is our job to understand this and do our best to ensure that every adaptation is a positive one.  I spoke about performance therapy - aka performance engineering - and that in a performance enhancement environment, that it may be important for us therapists to be able to wear many hats. Trent mentions this in a recent Q&A, that: “In many ways, the applied sports practitioner has to become an “expert generalist” being able to link and apply many interventions across many scientific disciplines to optimize performance.” Because we may often need – and therefore know how – to play the role of an associate coach."  I also suggested that everything we do should be athlete centered. That all interventions in a performance enhancement environment will have the end goal of performance enhancement (obviously), cognitive resiliency and injury prevention. The guiding framework and its application were discussed and in so doing, we must not be a be a slave to our methods. Being athlete-centered will minimize the opportunity for this. I spoke about three key components of dynamically assessing the athlete: the neuromusculoskeletal, the cognitive integrity, and the physiological. For the neuromusculoskeletal, I generally like to think of assessing along a static-dynamic continuum where I’ll start with watching the athlete in action (dynamic) in order to know what I see and what I don’t see, then progress along the continuum toward the static if I want to know why I don’t see what I don’t see. It is important though, that we have a standard operating procedure to be able to decipher what’s normal, when we expect it to be normal and when we expect it to be abnormal.  Dynamically, I will also want to understand – assess though interaction, observation, etc – the cognitive integrity and resiliency, or mental hardiness, of the individual since mindset always differs between individuals. Understanding athlete physiology is important as well since levels of stress may vary at any given moment in time. Therefore, how we intervene in their current state should be kept in consideration. Athlete monitoring comes to mind when it comes to physiology but in my opinion, just being present should be the top priority.  As I mentioned above, if every interaction we have with, and every intervention we give to, the athlete is considered a stressor that results in adaptation – positive or negative – then we need to “pick our battles” and intervene where we think is necessary rather than all the time. Manual therapy, in particular, can be a negative input on speed/power days or prior to competition if performed either too aggressively or in too high of a quantity. Additionally, we must time our recovery interventions as Joel Jamieson explains in this video. 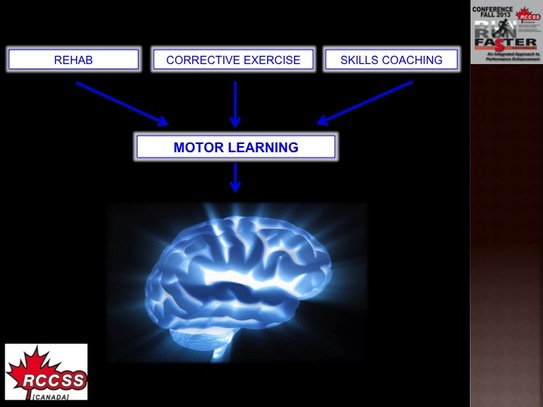 While many of the attendees at the conference were clinicians who specialize in clinical rehabilitation, part of my discussion was how we can implement traditional rehabilitation exercises into a performance enhancement environment. Especially during warm up and in general strength training circuits. Because whether it be rehab, corrective exercise, or skills coaching, my opinion is that it all falls through the filter of motor learning toward neuromechanical adaptation.  We do need to remember that there are two methods of attacking motor learning: 1) The Hard Disk via direct upload through automated subconscious control and the other; 2) The Working Memory via conscious control. Unfortunately, the latter – internally directed attention - often results in reinvestment (excessive conscious control of one’s skills) and may be more prone to breakdown in automaticity/fluency of performance through such means as paralysis by analysis so we must keep in mind that any of the techniques (physical or verbal) we employ can be positive or negative. And what we don’t want to achieve is paralysis by analysis.  Other methods to foster motor learning that I spoke about were implicit learning, good cueing and effective communication. Implicit learning is essentially presenting information at levels of perception below normal levels of awareness, whereby how we set up our intervention environment takes priority over verbal feedback. Again, verbal feedback can result in overthinking during motor executions and subsequently excessive conscious control of one’s skills. So often, we should STOP telling athletes what to do, LOOK – assess motor skills, and LISTEN to the athletes thoughts.  Effective communication essentially boils down to three main objectives: prevent paralysis by analysis, facilitate an optimal state of mind and readiness, and remove doubt. I shared my thoughts on effective communication through explaining what nocebos were (the same principles apply with Trent's Q&A above) and how we may be creating nocebos in our interventions. Again, we want positive adaptations and while many of us possess highly effective skillsets, it’s less about what we do and more about how explain it. Remember, it’s about the adaptation and it’s about what we leave behind.
I still think Steve Jobs was a genius, but if you look at the description beneath the video on the youtube page itself it says, "Technology codes our minds. Changes our OS" This got me thinking. With the advancement and abundance of personal technology devices, are we truly upgrading our neurological operating systems? In my mind, there's not doubt that new synapses are being formed and myelinated everyday but in a human sense, tradeoffs seem to be occurring. Is this "new and improved" OS of ours - the neurological software - actually taking up more space on our hard drives - the neurological hardware? Especially subcortically? Is a tradeoff occurring? Taken directly from the abstract of Kobesova and Kolar's recent paper, "Developmental Kinesiology: Three levels of motor control in the assessment and treatment of the motor system", we can see that: 'Following the newborn period, the subcortical level of the CNS motor control emerges and matures mainly during the first year of life. This allows for basic trunk stabilization, a prerequisite for any phasic movement and for the locomotor function of the extremities. At the subcortical level, orofacial muscles and afferent information are automatically integrated within posturalelocomotor patterns." Those of you who understand DK know that this is a critical period of learning. Not only physically, but socially, emotionally, etc as well (read "How Smart is Your Baby"). But strictly in a motor control sense, the obvious is that technology is making us more sedentary.
The not so obvious, is perhaps such technology is also rewiring our neurological OS - the subcortical, the automatic - and deleting our "movement" programs. Thankfully, we know that paper is still better. But my only hope is that we don't "empty the trash". In general, swimmers generally possess hypermobile shoulders. And by hypermobile, I mean greater than necessary ranges of motion and subsequently, often lacking synchrony of instantaneous neuromuscular firing in the scapulothoracic and/or glenohumeral joint regions. As a result, we know that since the body will always find the "easy way out", compensatory patterns and presentations commonly occur. And often, one of these presentations is reactive posterior cuff hypertonicity as a protective measure against further injury and/or pain. Whether it leads to bicipital tendon pathology, bursa irritation or other is besides the point. The main point, in my opinion, is why are some individuals still so enamoured by the sleeper stretch? I mean, for any given shoulder injury, presentation or diagnosis, out comes the sleeper stretch. In my mind, there's a difference between stiffness and hypertonicity. And sure, the glenohumeral joint "needs" adequate mobility. But perhaps more important, the GH joint needs dynamic, instantaneous neuromuscular control. And when we go to town with the sleeper stretch, we get sloppy. ESPECIALLY in swimmers! Because really, should we be treating the compensation or the cause? In a similar light, swimming mechanics incorporate both open and closed chain movements. Or in a Prague sense, alternating both support and stepping/grasping functions (read this article if you're unfamiliar with what I'm talking about). Now it's quite common for me to see corrective exercise prescription for the latter - YTWL's, theraband internal/external rotations, etc - but what I rarely see is the former. Coincidentally, here's a timely clip from Gray about motor control, stability and prime mover training: Because from the catch to (at least) the end of the pull falls under the "support function" category, in my opinion of course. And since this is the case, closed chain exercises should be the primary focus. Particularly if this is where mechanics are most faulty during skill execution.
So my recommendation to other clinicians is this... It's okay to think critically and ask yourself why. Why you are seeing what you are seeing. And why you are doing what you are doing. For those of you that have attended conferences with multiple presenters, you'll know that some conferences hold a Panel Q&A to wrap up the weekend.
Well recently I attended the Canadian Athletics Coaching Centre's National Throws Conference and one of the topics during the Q&A was feedback during competition. The panel included all the presenters and was moderated by Coach Derek Evely. Here are my notes on this particular topic: Feedback During Competition
|