|
EDUCATIONAL CONDUCIVITY "Refers to how easily a conference lends itself for learning. Specifically related to education, how conducive is a place or space for learning, creative thinking, problem solving, and decision making. To educate yourself you need to go to a space that promotes discussions at the bar and allows you to concentrate and surround yourself with professionals that are smarter than you." (modified from idea-sandbox.com) Year after year, Art Horne and the gang at the Boston Sports Medicine and Performance Group host their anual Summer Seminar. Having heard nothing but positive feedback from colleagues who have attended in the past, I decided that this would be the year to finally attend. Living in Western Canada, it certainly isn't easy to travel across the continent both from a time and financial perspective, but I felt that in order to continually better myself as a professional, attendance was a must. Like many of my previous educational endeavors, it was important for me to be 100% confident that this event was grounded in "educational conducivity" and not just a place where many of my friends were going to be. However, upon looking at the speaker lineup, it was more difficult to convince myself not to attend. 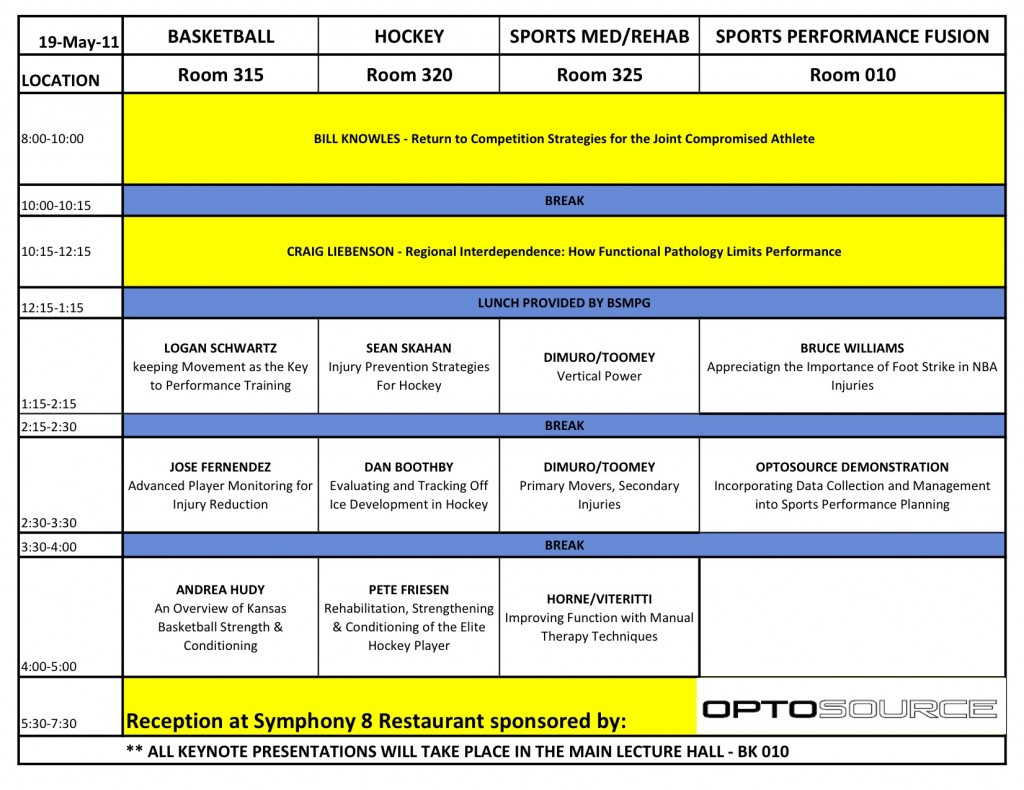 Day 1 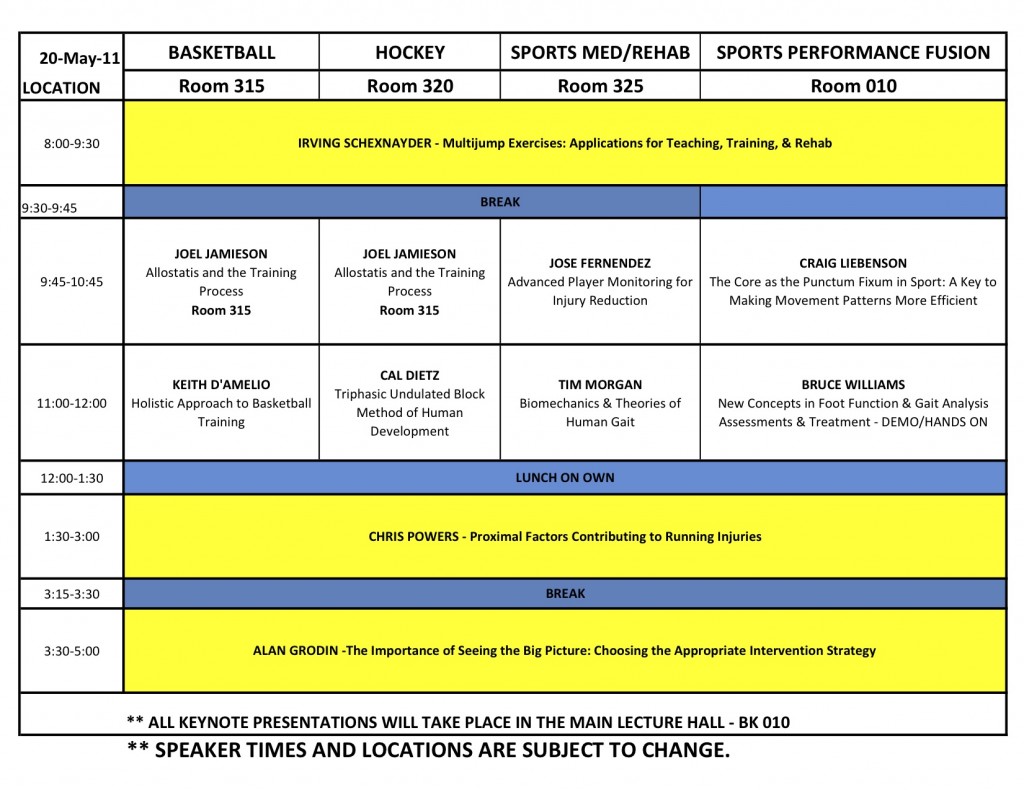 Day 2 Perhaps the most challenging task however, was deciding which sessions to attend. So aside from the keynote lectures where all delegates were present, I found myself attending lectures from the following: Sean Skahan, Dr. John DiMuro & Mark Toomey, Art Horne & Dr. Pete Viteritti, Joel Jamieson, and Keith D'Amelio. *Please note that while I was a note taking machine, I am going to limit this post to an informal, point-form summary of my synaptic moments. . Bill Knowles (Keynote) - "Return to Competition Strategies for the Joint Compromised Athlete"
Dr. Craig Liebenson (Keynote) - "Regional Interdependence: How Functional Pathology Limits Performance"
Sean Skahan - Injury Prevention Strategies For Hockey
Dr. John DiMuro & Mark Toomey - "Primary Movers, Secondary Injuries"
Art Horne & Dr. Pete Viteritti - "Improving Function with Manual Therapy Techniques"
Irving "Boo" Schenxnayder (Keynote) - "Multijump Exercises: Applications for Teaching, Training, & Rehab"
Joel Jamieson - "Allostasis and the Training Process"
Keith D'Amelio - "Solving the Performance Equation"
Chris Powers (Keynote) - "Proximal Factors Contributing to Running Injuries"
0 Comments
Leave a Reply. |