|
Quadrant 4 sport is a whole different ballgame. And over the past couple of years working with this demographic, I have come to learn and realize a few things that have not only changed my thought process but has also molded my approach to "therapy".
Sports Therapy
Performance Engineering
...this post was inspired by Stuart McMillan's post on performance therapy and ongoing commmunication with Patrick Ward.
0 Comments
Another case of Diastasis Recti again this morning. This time, in an athlete constantly reporting posterior shoulder tightness. I will admit that bad habits had taken the better of me recently whereby I had been dispensing "the band-aid" rather than looking for the cause of the bleed. But with the national championships coming up and the increasing importance of the need for optimal performance, it was important for me to look elsewhere. Looking back, it was easy to get into the trap of "releasing" the tight and symptomatic structures - and I do know better - but again, bad habits are easy to fall into. My bad. Most understand the importance of postural stability in the water for efficient streamlining and power generation but being in the "dynamic" end of the stability-motor control continuum, the lats should be relatively free and easy in the recovery phase and pre-catch. And in this case, they lacked the relative ability to dim down when necessary. Hence, the stiffness and tightness constantly reported posterior to the shoulder. Since the advanced DNS course last fall, Pavel Kolar shed some insight to the potential flaw behind the "lats as a 5th core muscle" way of thinking and in my opinion this is true especially if the demands of sport lie toward the left. 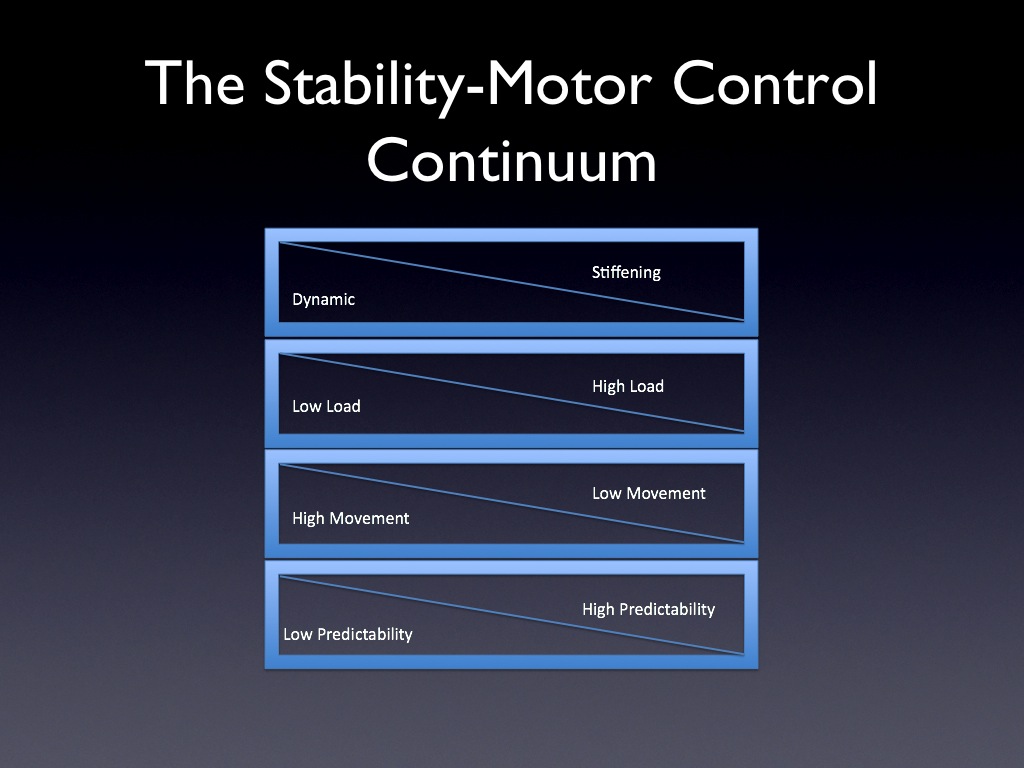 From this morning's assessment, my theoretical rationale for this was inefficient instantaneous intra-abdominal pressure as evidenced by the Diastasis Recti. Fortunately, with training this was able to be reduced but motor learning does need to take place and at this point, motor control has yet to be established.
It will be a work in progress, but I am confident that efficiency will be improved. It needs to since that's the nature of the beast with swimming. Although it seems - and I state this cautiously - that we collectively are improving our awareness of the role of diagnostic imaging in "painful" presentations, a recent encounter with an athlete reminded me of a different role.
The literature states that the correlation between positive findings on imaging studies and chronic pain presentations are likely weak at best but reality seems to state that patients still often search for that tangible finding that confirms their "pain". There are many causes of this I know, one of which is the "Nocebo" effect through clinician-patient communication, but I was recently reminded of a potential positive effect of an unremarkable or "normal" diagnostic imaging study. Let me frame this for you:
While I cannot explain the exact mechanism for this, I did ask Jason Silvernail if there was a term for this phenomenon. He wasn't aware of one but did state through our brief discussion that there was a "credible reduction of threat". Perhaps Fabrizio Bennedetti knows? He studies the neurobiology of placebos so while this isn't specifically a placebo or nocebo effect per se, maybe we can call it a "procebo"? Now, I'm certainly not advocating the use of diagnostic imaging for this purpose. However, this phenomenon does certainly interest me and do wonder what the literature says, if anything at all. In the meantime, if you're interested in what Dr. Bennedetti has to say, I recently listened to a great podcast with he and Dr. Ginger Campbell. Just a short post to share some ideas on "non-specific elbow rehabilitation". But before I proceed, I want to make it absolutely clear that I titled this "non-specific" simply because it can be incorporated in the rehab of several conditions...rather than suggesting that you diagnose elbow injury as "non-specific elbow injury".
Remember, as Andreo Spina suggests: "Specificity of Diagnosis = Specificity of Treatment = Specificity of Results" Anyway, several months ago I contacted James "Smitty" Smith to ask for his thoughts on grip training since he and his "crew" seem to be the go to guys when it comes to training this region of the body. My rationale for contacting him was not only for my own training but also because I felt that the commonly performed eccentric training of the flexors and extensors were just that, too commonly performed. In approaching "elbow" rehab, much of my work lately - while specific for each individual and certainly dependent on the assessment - has transitioned to incorporate the use of bottoms up kettlebell work for glenohumeral rhythmic stability and DNS protocols for upper quadrant resetting. However, thanks to Smitty's recommendations, I have now included the use of Fat Gripz, golf balls and thick rubber/elastic bands. Since we know from Craig Purdham and Jill Cook that not all elbow injuries (e.g. tendinopathies) require eccentric strengthening, here is a point by point framework of specific objectives of rehab and an example of corresponding strategies that I may use. Stability of the shoulder girdle
Flexor and Extensor Endurance
Grip strength
Cuff strength
Extensor Strength
Hamstring Injury Mini-Symposium by Karim Khan
Hamstrings Injury Prevention: An update by George Nassis
Fascia Science: Stretching the Power of Manual Therapy by Greg Lehman
 I had the pleasure of visiting the training facility of West Bromwich Albion of the English Premier League. Like a kid in a candy store, I was exited to visit and spend the day with Stephen Wright, the Lead Rehab Physiotherapist whom I met years ago at Athletes' Performance's Rehab Mentorship. To say that this visit was a privilege was certainly an understatement so rather than provide you with a summary, I thought it would be more appropriate to utilize a question and answer format to shed a little bit more light into their experiences and perspectives on sports science, strength & conditioning and rehabilitation. Especially given that there's only so much we can take away during spot visits. 1) Stevo, I cannot thank you enough for allowing me to spend the day with your team. Would you mind summarizing who comprises your support team, not including the coaches and scouting staff as well as the importance of the integration of all members? Well the Science and Medicine department is headed up by Dr Mark Gillett. He has a wealth of Sports Specific experience, has previously worked for Chelsea FC and is currently head of GB Basketball Science & Medicine team. It helps me immensely to work alongside a Dr who understands Physical Therapy and the rehab process. Then essentially we have a flat structure within the 1st Team Physical Therapy Dept each with a specialist area. The team consists of: myself – Lead Rehab Physio, Richie Rawlins - Performance Physio and Rick Carter – Part time Consultant Physio. In addition we are supported by two full time soft tissue therapists. 1st Team Sports Science is headed up by Chris Barnes, who works alongside 1st team Fitness Coach Matt Green and S&C Specialist Mark Jarvis, and who are supported by 4 sports science interns, and an IT intern. The Science and Medicine Team are further supported by part time Podiatrist, Osteopath, Nutritionist and Yoga instructor.  2) As the Lead Rehabilitation Physiotherapist, your obvious primary role is managing the care of their injuries. I was intrigued by the "Injury Progressions Board" you have posted in your rehab room. Without going into too much detail can you briefly summarize the impetus for this board as well as the importance of attaining the medical and sports sciences goals along the various phases? Sure I developed the Injury Progression board a number of years ago with a former colleague of mine Bill Styles (Celtic FC). He was a Sports Scientist who had recently joined us from another club, and we had to develop a successful working relationship quickly. So we basically sat down and hammered out what we thought each of our roles were in the rehabilitation process, and how they fitted in to the 4 basic stages of tissue healing (Hunter, 1994), namely: Phase 1 The time of injury, Phase 2 inflammatory (lag) phase, Phase 3 fibroblastic (regeneration) phase and Phase 4 the remodeling phase, and for each stage we agreed what our aims and objectives would be. We decided to add a 5th stage Monitoring and injury prevention strategies. Essentially whilst we both had a daily role to play in the rehabilitation of the injury, the Physical Therapist would lead the process in the earlier phases; where early goals could be accurate diagnosis, employ a PRICE strategy, review modifiable causative factors, screening data etc, leading to recovering full Range of Motion and pain free function during Activities of Daily Living, promoting a healthy injury site with optimal collagen formation, stimulate neuromuscular pathways etc. As we advance through the phases and the athlete was able to perform functional sport specific return to play drills, the role of the Sports Scientist increased, and progressed to be greatest during the latter stages at the extreme right hand end of the board where they player was required to perform all requirements of the game which their position demanded, repeatedly and in a fatigued state. The board gave us a simple checklist which ensured a safe appropriate progression based on successfully completing criteria for each phase. The Injury Progression board which you saw is quite simplistic, and whilst the phases and objectives continue to remain wholly appropriate, the influx of additional multidisciplinary staff, in conjunction with more sophisticated monitoring processes mean that there are many more strands feeding into a players rehab at any one time. In reality today we use a more comprehensive digital version of the board, which facilitates multiple disciplines to feed into each stage of the rehab process to create a pathway of care which is joined up, planned and has appropriate monitoring and goal setting built into it. An example of this may be graphical representations of objective markers, supported by progressive GPS, Accelerometry and Heart Rate monitoring. 3) You mentioned the "Yo-Yo" test. This seems similar, yet different, to the beep test. Can you explain it's relevance to soccer/football? Sure the standard Beep Test (Leger Test) requires the athlete to run between two cones placed 20m apart, at a steadily increasing pace, the pace is dictated by a beeping metronome which gets progressively faster, and upon reaching the mark the athlete turns around and runs back. It is a continuous run to failure. The Yo Yo Intermittent Recovery Test also requires the athlete to also complete a 20m run, turn around and run back in time to the increasing beep of a metronome, however after performing a shuttle they are allowed a 10sec recovery, before repeating the shuttle at ever increasing speeds. The intermittent nature of the Yo Yo test, together with the resulting higher speeds attained, mean that is of greater relevance in determining soccer specific fitness. A number of papers have found it to be a valid and reliable measure, and it would be an equally appropriate test for any field based sports requiring intermittent bouts of high intensity running (see paper below). Jens Bangsbo, F. Marcello Iaia and Peter Krustrup, (2008) The Yo-Yo Intermittent Recovery Test: A Useful Tool for Evaluation of Physical Performance in Intermittent Sports, Sports Medicine 2008; 38 (1): 37-51. 4) At this level of sport, you guys certainly have no shortage of "high-tech" equipement. Would you mind providing us with your experiences using the AlterG Anti-Gravity Treadmill and the Hydroworx pool? We have used the Alter G treadmills for 2 years now, and find them an invaluable tool for the load compromised athlete. This may be a fit player who is at a stage in their career where they cannot withstand high impact loading on their joints or tissues on a daily basis; or an athlete who is recovering from injury, where I find it removes some of the guess work associated with a graded return to full weight baring running. Amongst other things, running at lower percentages of full body weight like this clearly reduces the demand on the cardiovascular system, in situations where we want to increase the CV stimulus we have had a great deal of success in using it in conjunction with hypoxia, via a closed circuit bag and mask system and a hypoxic generator which is capable of simulating altitudes of up to 12 000ft . The hydroworx pool is a large underwater treadmill on a variable height floor, it allows us to simulate running, and perform multidirectional twists and turns in an off-loaded underwater environment. Similarly to above we use it to offload a compromised or injured athlete, but also find it an excellent medium for recovery sessions post match. The two pieces of equipment complement each other well, the Hydroworx enables the athlete to move freely, in an environment of increased hydrostatic pressure, and the Alter G allows us to more precisely grade external load acting on the body, albeit in a linear fashion. 5) I noticed your high altitude chamber, when exactly do you use this? This is our first season with the high altitude chamber. As you’ve seen it measures approx 100 square feet and contains a Woodway Curve treadmill, and an exercise bike. In the rehab process we may use it to increase cardiovascular stimulus in athletes who’s tolerance to load is compromised by injury, example sessions may include metabolic type circuits consisting of low load, high rep compound movements, or interval work on an ergo. Our S&C guru Mark Jarvis has coined the term hypoxing, to describe his much feared boxing sparring sessions which are brutal when performed at 10 000ft! The Sports Science team headed up by Chris Barnes have been exploring a variety of intermittent high intensity exercise protocols performed in hypoxic conditions, using amongst other things a non motorised woodway curve treadmill. Although this research is at an early stage, some of the results are impressive.  6) In speaking with Dr. Mark Gillet, your Head of Medical Services, he mentioned that your team has a "no tolerance" policy for groin pain. Can you shed some light into the importance of this? When Dr Gillett came on board 3 years ago he felt that the incidence of groin pain and training days lost to groin injury would be a key performance indicator for an English Premier League Medical Team. We have a low tolerance for withdrawing players from training with groin pain, and when withdrawn they undergo a repeat of our bespoke hip and lumbo-pelvic evaluation tool. The tool includes measures of groin strength in various positions, but is strongly focused on determinants’ of form and force couple closure of the pelvis, segmental stabilization, range of motion and symmetry. Our experience suggests that getting on top of these issues as soon as they arise, frequently allows a quick return to pain free training, and to date we have had very few if any players absent for more than a few days due to groin pain over a 3 year period, and zero incidence of sports hernia. It may be worth mentioning that whilst groin pain is often multi-factorial, and our assessment and interventions reflect this, we have observed a strong correlation with groin pain of poor extension control of the low back in football players for a number of years now. 7) Finally, your sports scientists, hold an important role on your team, especially in the analysis of load using such technology as GPS, Heart Rate and Heart Rate Variability monitoring and others. Would you mind providing us with some of variables you measure - as well as their importance - as they pertain to internal (cardiovascular) and external (mechanical) loads? Like many teams within the English Premier League, we use GPS, Accelerometry and Heart Rate monitoring to quantify training. Our Sports Scientists and interns crunch a vast amount of data which paint a picture of the nature and type of work done. Some of the commonly reported metrics which you will have seen us using will be: Total distance covered, no. of accelerations and decelerations, and these are self explanatory, although within this we have the ability to set thresholds or bands for what constitutes an acceleration or deceleration, and can tailor these thresholds to an individual. High Intensity Distance and High Intensity Time are measures of how much distance is covered or time is spent with the athlete moving above a particular speed. The software which we use to analyse these variables allows us to set this speed specifically for an individual. For example if you were one of our players Jeff, we may work out your running speed at lactate threshold, since above this velocity your blood lactate would increase and the effort or intensity would feel much harder, it may represent a useful threshold for what constitutes high intensity work for you as an individual. Alternatively you may have a good reason for selecting this threshold another way or as a percentage of you maximum speed. The main thing is that it is reflective of higher intensity bouts of work, and as such will be of greater value if the threshold is set specifically to you as an individual. Player load can be a very valuable metric. It is calculated using data acquired by accelerometers contained within the GPS unit. It gives you a single number derived from a complex calculation, which is reflective of how much movement a player makes in each of 3 planes, vertical, lateral and linear, and the calculation assigns a higher value to movements performed over greater range or those made at higher speeds. The player load gives you a metric which is measured in arbitrary units, but is reflective of effort. Different players will achieve differing loads for an identical task, depending largely on the efficiency with which they accomplish the task. To supplement this information we record Heart Rate data in the form of Red Zone minutes, time spent above 85% Heart Rate max, and something called a Training Impulse or TRIMP. To calculate TRIMP an exponential scale is applied to heart rate data as a percentage of Heart Rate max ie it assigns a greater value to Heart Rates which are closer to maximum than those closer to 50% on a 10 point scale. As such it creates a more complete picture of the overall cardiovascular workload than Red Zone minutes alone would. Our experienced staff closely monitor this data, along with a host of additional data streams, to establish trends over time which may be significant, ie markers of over-reaching or over training, injury or illness, fatigue or freshness, or performance. When a player is injured we refer to this information to tell us the precise physical requirements necessary for a given individual to play a particular position. During the rehab process we work to ever increasing percentages of these until we are satisfied that he can perform all of them and is safe to return. 8 ) Thank you Steve. I really appreciated the privilege of visiting and think you have a lot of information to share to sport medicine and performance professionals. You mentioned that you will be hosting a conference sometime next year. Can you leave us with some information that we should look forward to? Sure Jeff, building on the success of our 2012 conference, we are proud to announce that on March 20th - 21st 2013 we will be hosting a conference at the recently opened state of the art St. Georges Park, home of the National Football Centre in Burton-upon-Trent, Staffordshire, UK. The conference is titled Maximising Multidisciplinary Team Performance 2013: "The Success Factor", will host a world-renowned panel of experts, including Bill Knowles, Dr Greg Whyte, Calvin Morris, Humphrey Walters, Damian Hughes, Ian McCurdie, Nick Broad & others. We aim to explore the implementation, development and management of truly successful multi-disciplinary teams and how they can be harnessed to deliver sustainable world class sporting performance. In addition, myself, together with colleagues Dr Mark Gillett, Chris Barnes and Mark Jarvis will be taking the opportunity to further expand on some of the topics covered in this interview and share our experience with you. http://mdtconference2013.co.uk/ http://mdtconference2013.co.uk/wp-content/uploads/mdt2013-flyer.pdf  "It's not what you take when you leave this world behind you. It's what you leave behind you when you go." It seems like living the in the land of country music is starting to influence me a little. Well not really. But Randy Travis' quote from a really powerful song does have some relevance in both the medical and coaching fields. Although this isn't anything new, there's been a lot of chatter lately about "activating this muscle" or "releasing that structure". It is inherent in coaching, rehabilitation and manual therapy, no doubt, but what are the ramifications of this type of discourse? In my opinion, I don't think this is a good thing. Not now, and not for the future. And I can certainly emphasize with Jason Silvernail when he previously stated, "for crying out loud don't give patients a giant nocebo by telling them they have fascia restrictions, inhibited muscles, or joints out of place. Because then I have to explain to them that that's not accurate. And that's exhausting. It's less about what you do and its more about how you explain it ". I have been a strong advocate for the improvement of communication skills over the last year or so. Perhaps I need to start a foundation or something. But in all seriousness, the way we communicate both on a personal (in practice) and a societal level (on the internet) can truly either positively or negatively affect what we leave behind. Put it simply, it's called a nocebo. And Paul Enck wrote about this nocebo in the New York Times recently. It's a nice read to give you a good idea of what I'm talking about. But more importantly he states, "A doctor's choice of words matters...The nocebo effect presents doctors...with an ethical dilemma: on one hand, they are required to tell patients about the potential complications of a treatment; on the other hand, they want to minimize the likelihood of side effects. But if merely telling patients about side effects increases their likelihood, what is to be done? Better communication is the answer. When talking with patients, doctors...often say things with unintended negative suggestions, like “it’s just going to bleed a bit” or “you must avoid lifting heavy objects — you don’t want to end up paralyzed.” We recommend more extensive training in communication for doctors and nurses, to help them use the power of their words appropriately. As the great cardiologist Bernard Lown once said, “Words are the most powerful tool a doctor possesses, but words, like a two-edged sword, can maim as well as heal.” The nocebo isn't only about side effects of treatment, mind you. In fact, it often pertains to the positive effects of treatment. "Activating this muscle" and "Releasing that structure". This is exactly what I'm talking about. Because the next time an individual experiences pain attributed to a similar region of the body, they're going to think that they need this released or that aligned. Give this post a read. It may shock you or it may not. But one thing I'm almost positively clear about is that one's back is never out and their leg length is fine. Now all of this can be applied to coaching and rehabilitation as well. Many of us have heard of "paralysis by analysis". And again, it's not what you take - or do - it's what you leave behind. Because if you're telling someone to "activate your glute" or more subtly "feel it in your glute", what you leave behind may not be a good thing. This is called "attention focus". You can read more about it here, listen to some of Nick Winkleman's podcasts on strength coach or read Gabriele Wulf's work directly. The AIS also has a nice article on coaching strategies to minimize paralysis by analysis as well. Ultimately, you can still keep doing what you're doing. I'm not asking you to stop. But what I'm asking you to do instead - much like Foucault in his writings about power and discipline - is to think more carefully, critically and responsibly about the effects your practices might be having... ...and what you're leaving behind.  “People know what they do; frequently they know why they do what they do; but what they don't know is what what they do does.” - M. Foucault If you have ever trained hockey players, you will no doubt know that these athletes have distinct early sprinting mechanics. Many possible factors may contribute to this biomechanical presentation, from overloaded lumbar extensors and an anterior pelvic tilt to stiffened posterior chains and external hip rotators. However, one thing I have failed to extensively consider until know was the effect of skating mechanics to sprinting mechanics. Looking closely at one of Endeavor's hockey players above (the athlete on the right), you will notice a distinct eversion of the calcaneus and external rotation of the tibia that is not uncommon in this population while sprinting. Likely a mechanical adaptation through many years spent on the ice, hockey players must utilize increased external rotation of the hip and tibia to compensate for decreased calcaneal eversion secondary to restrictions from the utilization of skates (both skating mechanics and wearing a boot) on the ice. As Frans Bosch states in his book, "Skaters cannot rotate on the blades of their skates, and consequently must avoid everting the heel during push off. They cannot make use of the possibility for lateral rotation in the lower leg because it will be impossible to develop medial rotation which is needed during pushoff. In order to direct sufficient force of thrust toward the rear during the start, the foot must still be everted as it is placed on the surface. To solve this, the skater will begin by rotating the hip strongly laterally so that the knee is pointing further outward during the first part of the start than is customary for the runner". The way I see it - and I'm open to be corrected as this is merely a hypothesis - players have adapted in a manner whereby through the advantage of utilizing increased hip external rotation on the ice, they subsequently have a decreased ability to control the eccentric forces in eversion/dorsi-flexion during the early phases of sprinting - resulting in overload in the deep compartment of the medial lower leg.
While this adaptation may not result in foot and ankle dysfunctions for some, because many young hockey players sprint during dryland training and / or take up other sports in the off-season or when they retire, it is not uncommon for them to experience lower leg overuse injuries. Medial Tibial Stress Syndrome and Tibial Stress Fractures are two such injuries. So what can we do about it to better control eversion and subsequently prevent injuries? My suggestions are as follows:
Again, the above is merely a hypothesis and I will admit that I have yet to look deeply into the research to investigate whether or not this has been researched. But to me it makes sense and for now, I am going to run with it. I have had a little bit of a reality check of late. Coming into the new varsity season, I had grandios plans for the athletes whom I have to privilege of working with. Stress questionnaires, HRV monitoring, and everything in between. Unfortunately, what I forgot to realize was that before you get to point D, you need to make sure you hit points A, B and C first. I was stepping up to the plate with the intention of hitting a bomb. But what I really needed to do was take care of my own backyard. But unfortunately, I lost a little sight of the "as little as necessary" principle. Because reality is:
And what I really needed to do was, as Coach Wes Moerman puts it, "Do the common things uncommonly well" So to me what that means, is emphasizing the smooth running of the day to day operations but keeping the big picture in mind. And in a low tech environment, that means ensuring that your athletes are
Coach Boyle mentioned in a recent podcast, "Do the best job you can, where you are, with what you have" That all said, monitoring is very important. But again, athletes are not robots and sometimes we must take a Foucaudian approach to sports performance. So if you have the luxury of incorporating the high tech, please do so. But do make sure it doesn't replace knowing and communicating with your athletes regularly. And if I may suggest, the "interactor" approach be utilized over the "operator" approach.
And truly, it won't get any simpler. |